



The Twitter account of Donald Trump Jr was suspended yesterday for promoting a video tweet by an African medical practitioner in the US who claimed that hydroxychloroquine works as a treatment for the COVID-19.
While the video was also retweeted by US president Donald Trump, his own account was not suspended because he did not upload the video but only retweeted it.
Twitter has taken a noticeable stance against misinformation about the COVID-19, rolling out a series of new features aimed at identifying and curtailing fake tweets about the virus. The warning labels, fact-checking labels, and outright removal of misleading tweets are ways the social media platform has been tackling misleading tweets about the COVID-19.
According to the video responsible for the suspension of Trump’s eldest son, a mixture of hydroxychloroquine, Zinc, and Zithromax has been used to cure about 350 patients in the States. The video also claimed that wearing of masks is not needed.
Both claims are in direct conflict with WHO’s viewpoint that prescribes wearing of face masks as an effective measure in curbing the spread of the virus. WHO also warns that hydroxychloroquine has not been known to produce any anti-viral effect where the coronavirus is concerned.
The video has however made the rounds on Twitter, Facebook, and Youtube, and has reportedly gathered more than 20 million views already.
Time factor in the fight against COVID-19 misinformation
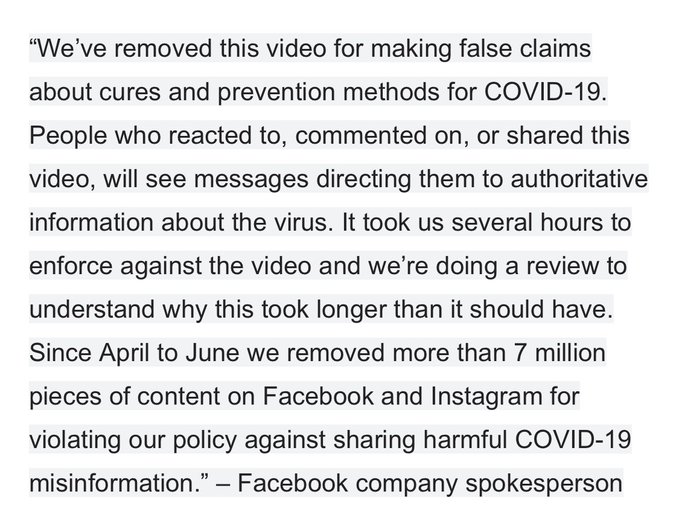
All three platforms have removed the controversial video from their platforms, but not before it gained significant traction. It already had about 18 million engagements from Facebook alone before catching the attention of the social media giant and getting pulled down.
While Facebook says it removed over 7 million misleading posts between April and June, the time it takes for a fake news post to catch its attention reduces the effect of the censoring by the time it eventually happens.
There is also the case of other videos or posts springing up from the original misleading post concerning the COVID-19. This has been the case with Stella Immanuel’s post which has led to other videos and content that are similar to hers being created and shared on Twitter, Facebook and other platforms.
As much progress as these platforms have made in the effort to curb fake news, the news keeps spreading. This is partly because social media users keep repurposing and resharing the content as if they are determined to see just how many posts the social media platform can eventually take down.
Besides Twitter, Facebook and YouTube, Whatsapp is another thriving platform for fake information about the COVID-19. While what is trending can be easily noticed and called out by users of platforms like Twitter and Facebook, the same is not so easy with Whatsapp.
Being a more personal platform, misleading content may have been broadcast to numerous WhatsApp groups and contacts and the viewing will be at the sole discretion of the receivers. This is more so because only the sender of a content has the choice to delete it from the view of every other person on the group, except the receivers choose to delete it individually from their feed.
Therefore, while some efforts are being made on Twitter and Facebook, not much is being done to curb the spread of fake or misleading news about the COVID-19 on Whatsapp.
Social media posts by medical practitioners; information or misinformation?
A question that arises with social media platforms censoring content is that of authority. In this case, what empowers a social platform to censor the medical opinions of a medical practitioners? The only plausible reason is that the tech platforms are making their judgement based on the recommendations and guidelines of the World Health Organisation.
There are various stages for a proposed drug to pass through before acceptance as treatment for a given illness. For hydroxychloroquine which is already certified for consumption, the most important phase is Phase 3 which stipulates that the drug be administered to a large trial group of between 300-3000 patients suffering from the illness it is been tried for.
Thus, while there is no study involving this amount of sample size to determine hydroxychloroquine’s real efficacy, there are studies that prove it doesn’t work. The latest result of such a study was released in June by the Randomised Evaluation of COVid-19 thERapY (RECOVERY) after its trial on hydroxychloroquine.
The study involved more than 4,000 patients from 175 hospitals in the UK. According to the chief investigators, Prof Peter Horby and Prof Martin Landray;
A total of 1542 patients were randomised to hydroxychloroquine and compared with 3132 patients randomised to usual care alone. There was no significant difference in the primary endpoint of 28-day mortality (25.7% hydroxychloroquine vs. 23.5% usual care; hazard ratio 1.11 [95% confidence interval 0.98-1.26]; p=0.10). There was also no evidence of beneficial effects on hospital stay duration or other outcomes.
“These data convincingly rule out any meaningful mortality benefit of hydroxychloroquine in patients hospitalised with COVID-19.”
Still, the professional opinions of a medical practitioner is not something that deserves to be discarded and maybe deserves to be seen and tested and proven to be wrong (or right). In the case where it has the propensity to mislead people and cause damage however, taking down posts becomes as important as freedom of speech.
